
What's the Difference Between EHR Data Migration and Data Conversion?
When healthcare organizations start planning an EHR transition, two terms come up almost immediately: "data migration" and "data conversion." Most people use them interchangeably, which is understandable.
They're related, they often happen at the same time, and vendors don't always help clarify the distinction. But treating them as synonyms can lead to real gaps in planning, budget surprises, and, in the worst cases, data loss that affects patient care.
Whether you're an EHR vendor onboarding a new practice to your platform or a practice administrator overseeing a system switch, understanding what each process entails helps you ask the right questions, set realistic expectations, and choose the right partner. This guide breaks both terms down in plain language, explains when each applies, and walks through why the difference genuinely matters in the context of clinical data.
Navigating an EHR transition?
Defining the Terms (Without the Jargon)
Before diving into comparisons, it helps to anchor the definitions with something concrete.
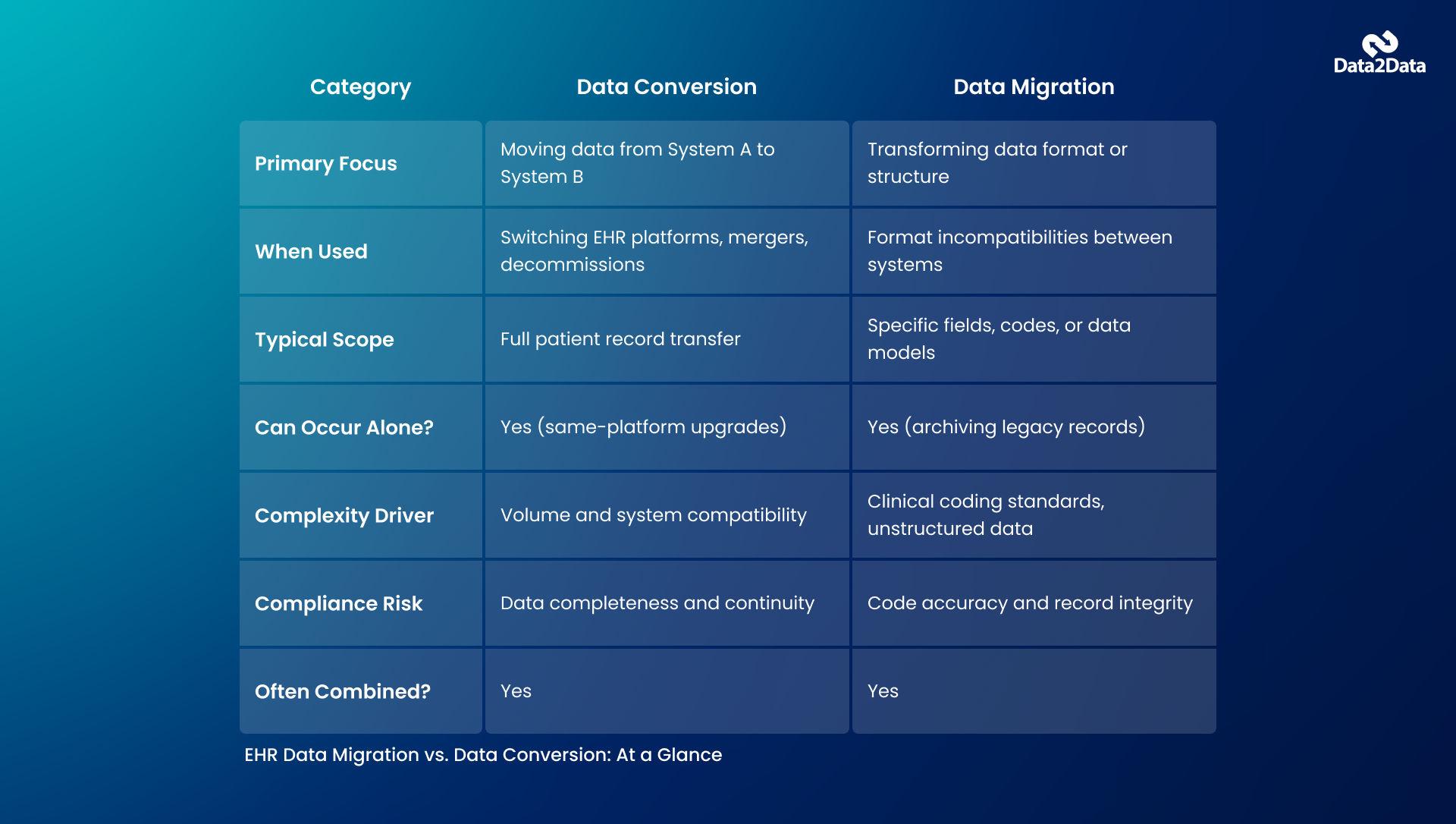
EHR data migration refers to the process of moving patient data and clinical records from one system to another. Think of it as a physical relocation: you're moving everything that lived in System A to System B.
Migration typically happens when a practice switches EHR platforms, merges with another organization, or decommissions a legacy EHR system.
EHR data conversion, on the other hand, is specifically about transforming the format or structure of data to make it compatible with the destination system. Data stored in one EHR may follow a completely different data model than the one it's heading to. Conversion is the translation layer that enables compatibility.
Here's a straightforward analogy. Imagine you're moving from one home to another (migration), but your new home uses a different electrical system than your previous one (conversion). You don't just move the appliances; you have to rewire or adapt them so they function in the new environment. Both steps are necessary, but they're distinct jobs requiring different expertise.
Why These Two Processes Are Often Confused
The confusion is largely practical. In most real-world EHR projects, migration and conversion occur in tandem, and vendors sometimes bundle them under a single label, such as "data migration services" or "EHR transition support." That bundling isn't wrong per se, but it can obscure which activities are actually being performed and who's responsible for what.
A few scenarios help illustrate when each term is the right one:
- Upgrading within the same EHR platform primarily needs migration: the data structures are similar enough that format transformation is minimal.
- A small practice moving from a proprietary legacy system to a cloud-based modern EHR often needs substantial conversion work because the data models are fundamentally different.
- An EHR vendor onboarding a new client from a competitor's platform almost always needs both: the data must be extracted, converted to a compatible format, and then migrated into the new system.
Understanding which scenario applies to your situation shapes your entire project plan, from timeline and staffing to vendor selection and risk management.
What Happens During EHR Data Migration?
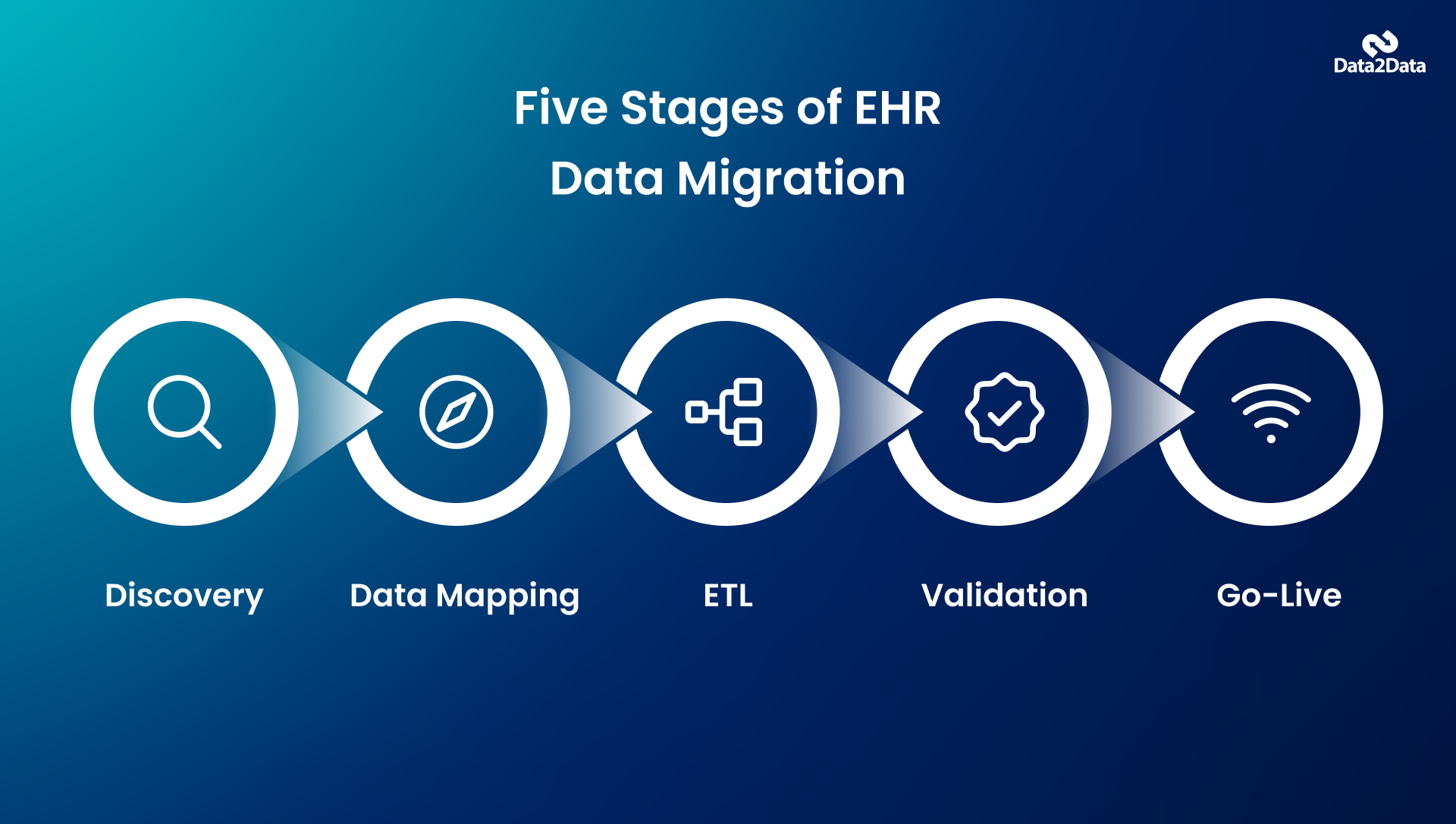
A well-executed healthcare data migration project follows a structured process. It's rarely as simple as exporting a file and importing it elsewhere. Here's what the process generally involves:
Discovery and scoping
Before anything moves, the team needs a clear inventory of what data exists, where it lives, what format it's in, and what the destination system expects. This phase often reveals surprises: incomplete records, duplicate entries, or data stored in formats the target system can't read.
Data mapping
This is where migration and conversion overlap most directly. Data mapping defines how fields in the source system correspond to fields in the target system. If the source system stores patient allergies in a free-text field, but the target system expects structured codes, that gap must be addressed through conversion logic during the mapping phase.
Extraction, transformation, and loading (ETL)
The data is extracted from the source, transformed to meet the target's requirements, and loaded into the new system. ETL is where the technical work happens, and it's where experienced healthcare data specialists earn their keep. This phase requires both technical depth and clinical domain knowledge.
Validation and testing
A patient data migration project isn't complete until the data in the new system is verified for accuracy, completeness, and integrity. This phase typically involves running comparison reports between the source and target, reviewing sample records, and having clinical staff confirm that records look right.
Go-live and post-migration support
After the cutover, issues tend to surface. A reliable EHR migration partner provides support during the initial weeks to address data anomalies before they become operational problems.
What Makes Data Conversion Complex in Clinical Settings
Clinical data is among the most complex data categories to convert. A few factors make it uniquely challenging:
Unstructured content
A significant portion of clinical documentation is in the form of free-text notes, scanned PDFs, and dictated narratives. Converting this type of content into structured, queryable data in a new system requires intelligent parsing, manual review, or both. There's no shortcut here.
Coding and terminology standards
Healthcare data rely on coding systems such as ICD-10, CPT, SNOMED CT, and HL7 FHIR. When a source system uses one version of a code set and the destination expects another, the conversion must accurately map codes. Mismatched codes don't just create administrative noise; they can make clinical data meaningless or, worse, misleading.
Regulatory requirements
Data management in healthcare is more than a technological issue. It entails certain legal requirements. One of the main provisions of HIPAA states that patient information must be available and accurate during the conversion from one system to another.
This is why generic IT firms rarely succeed with clinical data projects. The domain knowledge required to handle medical coding, understand clinical workflows, and anticipate data quality issues is highly specialized. It's a primary reason why practices and EHR vendors seek out partners with deep EMR data migration experience rather than general database migration services.
More detail on Data2Data's service approach: data2data.com/services
When You Might Need One Without the Other
Most EHR transition projects involve both migration and conversion, but not always. A few situations where one may occur without the other:
Migration without significant conversion
Moving from one version of an EHR system to another does not necessarily involve significant changes to data structure, as the models are consistent. However, it involves moving some data, which requires a little rework. This is mostly an issue of logistics, not technology.
Conversion without migration (Data Archiving)
Some practices do not need all historical data to be transferred to the new system; rather, they require archiving legacy records in a manner that makes them accessible and usable for any compliance-related issues. This is essentially the process of converting legacy data into a more easily accessible form.
This second scenario is where Data2Data's
CareArchiver platform is purpose-built to help. Rather than paying ongoing licensing fees for a legacy system just to maintain read access to old records, practices can archive that data in a structured, HIPAA-compliant format. It's a cost-effective alternative to a full migration for organizations that need historical data preserved but not actively used.
The Cost of Getting This Wrong
This is the part that decision-makers need to take seriously.
When migration and conversion are not properly planned and scoped as distinct activities, projects tend to go sideways in predictable ways:
Data loss
If conversion logic isn't thoroughly tested before migration begins, data elements that don't map cleanly can simply drop out of the process. In a clinical context, a missing allergy or an incomplete medication history is a patient safety issue.
Timeline overruns
Discovering mid-project that a large chunk of source data is in an unsupported format pushes go-live dates back, sometimes by months. That delay carries real cost: staff overtime, duplicate system licensing fees, and productivity loss during a critical operational period.
Post-go-live cleanup
Some organizations move first and clean up later. This approach leads to months of post-migration remediation work that's far more expensive than proper upfront planning would have been, and it erodes clinical staff confidence in the new system.
Compliance exposure
Records that were accurate in the legacy system but became garbled or incomplete during conversion can create audit risks. For practices subject to CMS reporting or HIPAA audit readiness requirements, this is not an abstract concern.
The organizations that get EHR transitions right are those that engage a partner with genuine depth in healthcare data management early in the process, before the scope is set and before contracts are signed.
Choosing the Right Partner for Your EHR Data Project
Whether you're an EHR vendor managing client onboardings at scale or a practice administrator overseeing a single system switch, the partner you choose for clinical data conversion and migration matters as much as the platform itself.
Here's what to evaluate:
- Healthcare-specific experience: Firms with 20-plus years of working directly with EMR and PMS data structures understand what general IT consultancies miss. The nuances of clinical data, from HL7 message formats to payer-specific billing codes, require genuine domain expertise.
- Full data lifecycle coverage: The best partners handle more than just migration. Look for a team that covers extraction, conversion, integration, analytics, and healthcare data archiving under one roof. Fragmented vendor relationships create coordination risk and accountability gaps.
- Boutique service model: Mid-market practices and growing EHR vendors often get lost in the queue at large IT firms. A partner with a boutique service model gives you direct access to senior data specialists rather than handoffs through support tiers.
- Proven validation methodology: Ask specifically how a prospective partner validates data integrity post-migration. Vague answers are a red flag. Look for specifics: reconciliation reports, record-level sampling, and clinical staff sign-off built into the process.
Data2Data has spent more than two decades working exclusively in healthcare data, partnering with both providers and EHR vendors to manage the full spectrum of data projects. Our team has hands-on experience with the data structures behind systems like Epic, eClinicalWorks (eCW), AdvancedMD, Cerner, AthenaHealth, Tracknet, Practice Fusion, NextGen, and over 120 other EHR platforms, as well as various pharmacy software solutions.
Final Thoughts
The distinction between EHR data migration and data conversion isn't academic. It shapes how projects are scoped, how risks are identified, and whether the data your clinical teams rely on arrives at the new system intact and usable. Getting clear on these concepts early in your planning process puts you in a far better position to evaluate vendors, build realistic timelines, and avoid the costly surprises that derail too many EHR transitions.
If you're in the early stages of planning a transition or helping a client navigate one, Data2Data brings the experience and full-service depth to handle it right. Explore our services or reach out to our team to talk through your specific situation.
Expert guidance for your data project
Frequently Asked Questions
What is the difference between EHR data migration and EHR data conversion?
Migration refers to the act of moving data from one system to another. Conversion refers to transforming the format or structure of that data so it's compatible with the destination system. In most EHR transition projects, you need both: the data must be converted to a compatible format before or during the migration. The distinction matters because it requires different technical approaches, timelines, and validation steps.
Do I always need both migration and conversion when switching EHR platforms?
Not always, but usually. If you're upgrading within the same EHR ecosystem (for example, moving from one version of a platform to a newer release), the data structures are often similar enough that significant conversion isn't required. However, if you're switching from one vendor to another, especially from a legacy system to a modern cloud-based platform, both are almost always necessary. The degree of conversion work depends heavily on how different the source and target data models are.
How long does a typical healthcare data migration project take?
Your legacy EHR records must remain accessible for the duration of your legal retention obligations, which vary by state but often extend for seven to ten years or more. Rather than maintaining the live legacy system (which is expensive and creates ongoing security exposure), most organizations use a clinical data archiving solution to preserve and provide compliant access to those records.
How do we verify data accuracy after the migration?
Data accuracy depends on the rigor of your mapping and validation process. A thorough migration includes source-to-target reconciliation reports, user acceptance testing with real migrated data, and documented sign-off from clinical and administrative stakeholders before go-live. Working with a partner who has experience with your specific legacy platform significantly reduces the risk of mapping errors.
